A 75 year old female with SOB and weakness
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs". This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
This is a case of 75 year old female house wife, who was brought to the casualty yesterday on 4/11/22 with the chief complains of
Shortness of breath since 10 days
Decreased appetite since 4 days
History of presenting illness:-
Patient was apparently asymptomatic 5 years ago, then she developed sob and was taken to a private hospital , was diagnosed with bronchial asthma , where she was given nebulisation and medications on which it was symptomatically relevied.
Since then she had been using MDI
Since 2-3 years she stopped using MDI and on medications for releif
6 months back, Patient developed similar complaints with fever and was admitted in a private hospital where it was treated as Bronchial asthma
10 days back she developed sob grade 3 (mmrc)- insidious onset, gradually progressive associated with cough - Non productive and fever.
Not a/w chest pain ,wheeze, palpitations, sweating
No h/o orthopnea , PND
She was given nebulisation 5 days back to relieve her symptoms temporarily
3-4 days back patient again developed sob (grade 4) her sob exacerbates in winter seasons.
Decreased appetite since 4 days
Dysphagia since 2-3 days which was progressive and more to solids than liquids
She was then taken to a local hospital in view of decreased appetite and dysphagia, weakness , increased fatigue, hypomentation , delayed response, but obeying commands, unable to move from bed or walk without support
4/12/22 morning-
She was taken to miryalguda hospital- with increase in severity of sob and weakness.
Was investigated and referred here.
Widal test done

Past history-
history of fall (head injury) 10 years ago
not associated with loc, projectile vomiting , seizures, weakness
Ct brain was done
She was then diagnosed to be having hypertension and was started on Telma H
4 years back- patient diagnosed with hypothyroidism (using thyronorm)
N/k/c/o DM, CAD, TB ,epilepsy
Daily routine of the patient -
She gets up at around 6 am in the morning, eats her breakfast made by one of her family members. She stopped cooking 5 years ago. Patient stays in a closed room alone most of the times.
Her lunch around 1:00pm afternoon includes rice and curry or dal predominantly.
She takes nothing for snacks
Dinner rice and curry at 9pm
Patient's life style is predominantly sedentary with minimal physical activity
Family history- no h/o similar complaints in her parents
her son was an asthmatic (died 8 years ago).
Personal history-
Diet - vegetarian
Appetite- decreased
Sleep - adequate
Bowel and bladder regular
No Addictions

Drug history-
Patient is on tab. Montelukast (OD)
Tab. Prednisolone (OD) since 5 years.
Allergy history
No h/o allergies to food dust and pollen.
General physical examination-
Patient is concious coherent, not cooperative well oriented to time place and person
Consent of patient was taken before examining her.
Vitals - at time of presentation
RR- tachepnic
GCS- E4V5M5
BP- 110/70 mm Hg
Saturation O2- 89 on RA
96 on 2lts O2
Grbs-141 mg /dl
PR- 120 bpm , irregular
Pallor present

No icterus cyanosis clubbing lymphadenopathy & pedal edema
Systemic examination-
Respiratory system-
On inspection-
Shape of chest - elliptical
Chest appears to be b/l symmetrical
Trachea appears to be central
Chest expansion is symmetrical
(Slightly appears to be hyperinflated)
Supra clavicular hollowness seen on the right side
Apical impulse not seen


Palpation-
All inspectory findings confirmed
No local rise of temperature
No tenderness
Trachea is central
Chest expansion equal on both sides
Tactile vocal fremitus- equal on both sides
Dimensions-
Chest circumference 72 cm
Hemithorax - 36 cm
Anterior posterior 20 cm
Transverse 32 cm
Ratio is 0.625
Percussion-
All lung fields are resonant
On Tidal percussion-
Inspiration dullness in right 6th ICS
Expiration- dullness on right 5th ICS
Auscultation-
B/l airway entry present
Coarse crepitations on inspiration and expiration heard in inframammary and infraaxillary area.
Fine crepitations in inframammary area
Mild wheeze on expiration
Rhonchi and coarse crepts heard in infraclavicular area
CVS-
Apex beat felt and auscultated in left 5th ICS MCL
S1, S2 heard
No murmurs
CNS
Higher mental functions- intact
Sensory system intact
Motor - bulk normal
Tone normal
Reflexes
Upperlimb biceps 4/5 right &left
Triceps 4/5 right &left
Supinator 4/5 right & left
Lower limbs-
Knee jerk+
Ankle jerk+
Abdomen-
Shape scaphoid
No scars and sinuses
No organomegaly
Bowel sounds heard
Investigations-
CBP-

Hb- 10.1
Tlc- 18.5k
Plt- 3.32lac
Serum electrolytes-
Na- 123 meq/l (hyponatremia)
K- 3.3 ( Hypokalemia)
Cl- 82 (hypochloremia)
Serum osmolarity - 254 (hypotonic)
Urine-
Na- 125
K-26.9
Cl-149
ABG-
PH- 7.54
PCo2- 27.8
PO2- 61.6
SpO2- 93.5
Hco3- 26.3(st) 23.8(c)
(metabolic alkalosis)
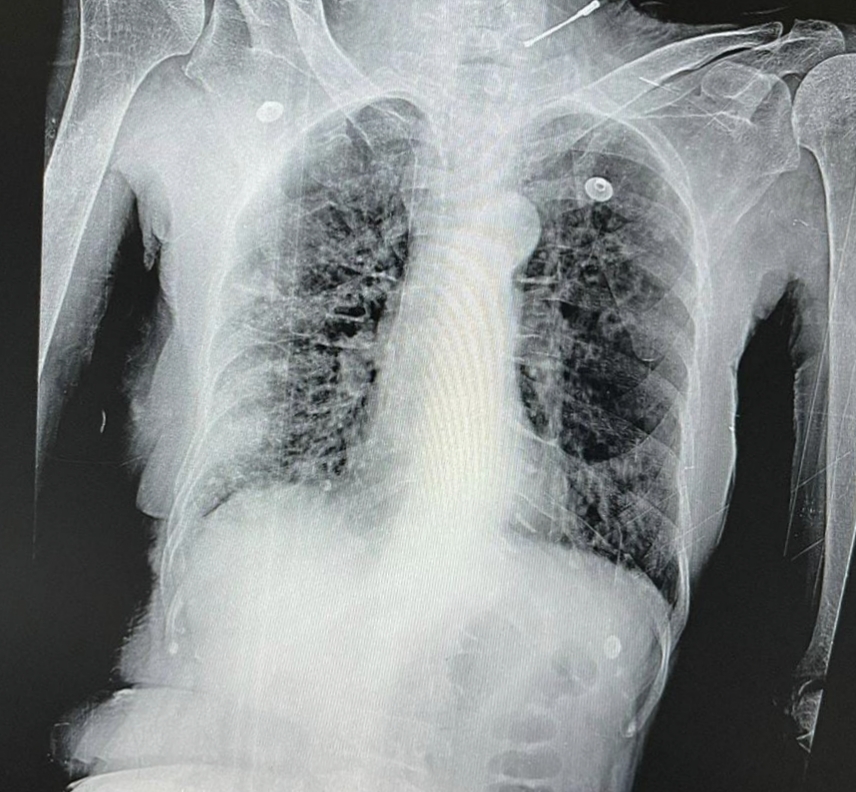
CXR-
Showing increased broncho pulmonary vascular markings
Pleural thickening
Tubular heart
Reticular pattern suggesting ILD
ECG -
On 4/12/22-

On 5/12/22-

Provisional diagnosis-
Acute exacerbation of Asthma, COPD? Miliary TB? ILD?with hypertension and hypothyroidism
With Hyponatremia, hypokalemia under evaluation
Treatment:
O2 inhalation with 2-4l/min
Inj. Augmentin
Inj. Pantop
Nebulisation with duolin and budecort
Syr. Potklor
Syr. Aristozyme
Tab . montec
Discussion-



Comments
Post a Comment