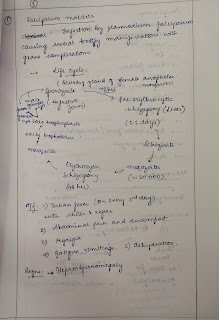
A 14yr old boy with fever lymphadenopathy and peripheral cyanosis
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs". This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
This is a case of 14 year old boy resident of Narketpally who was admitted with the chief complaints of -
Fever since 14 days
Loose stools since 14 days
Vomitings since 14 days
Bluish black discoloration on tips of fingers since 11 days
History of presenting illness:
Patient was apparently asymptomatic 14 days ago then he developed high grade fever sudden in onset, gradually progressive, evening rise of temperature, associated with chills and rigors, generalized weakness and fatigue and not releived on medication.
Cervical, inguinal lymphadenopathy was noticed
No h/o weight loss, night sweats
Loose stools since 14 days, watery, foul smelling, non blood stained, around 4-6 times a day
Vomitings since 14 days, immediately after solid or liquid food intake,non projectile,bilious, non foul smelling non blood stained, food as content
Yellowish discoloration at the tips of fingers since 14 days, turned to bluish since 12 days and bluish black since 11 days. Burning sensation over the palmar surface of both the hands.
Past history:
H/o trauma to
No h/o similar complaints in the past
No h/o blood transfusions
No h/o HT DM asthma TB
FAMILY HISTORY:
No similar complaints in the family.
Personal history:
Diet- mixed
Appetite- normal
Bowel and bladder movements- Regular
No Allergies
No Addictions
General physical examination:
Patient is concious coherent and cooperative well oriented to time place and person
No pallor


No icterus, clubbing, lymphadenopathy, cyanosis
Vitals:-
Temperature:
RR
BP
HR
Systemic examination:-
CVS-
Inspection:
shape of chest wall- elliptical
No scars, sinuses, visible pulsations
Palpation-
No thrills heave felt
Apical impulse palpable at left 5th ICS along midclavicular line
Percussion:
Heart borders percussed- no abnormalities noted
Auscultation:
All areas of heart auscultated
S1, S2 heard no murmurs heard
Respiratory system:
Shape of chest - scaphoid
Movements of chest wall - b/l symmetrical expansion with respiration
No scars sinuses
Trachea - central
Normal vesicular breath sounds heard
GIT:
Shape of abdomen- scaphoid
No scars, sinuses, visible pulsations
No tenderness in quadrants of abdomen
Soft, no organomegaly
Bowel sounds heard
CNS:
NFND, power tone normal
Reflexes present


Comments
Post a Comment